















Editor’s Note: Peter Bergen is CNN’s national security analyst, a vice president at New America and a professor of practice at Arizona State University. He is the editor of the Coronavirus Daily Brief and author of the new book “Trump and His Generals: The Cost of Chaos.”
Infectious disease expert Michael Osterholm, who has been warning for a decade and a half about the possibility of a global pandemic, said the coronavirus we’re fighting is at least as infectious as the one that killed an estimated 50 million people in the 1918 flu worldwide outbreak.
He said we’re only in the second inning of a nine-inning contest, with the possibility of as many as 800,000 deaths or more in the US over the next 18 months.
Osterholm also pointed to a shortage of chemical reagents that are necessary for widespread testing for the virus and said that the CDC’s low public profile in this pandemic in the United States has been a “tragedy.”
He decried the lack of a national long-term strategy for the pandemic and noted that there are real questions about the efficacy of the antibody tests that are being developed to detect if people have been exposed to the virus.

Osterholm, who founded the University of Minnesota’s Center for Infectious Disease Research and Policy, warned in 2005 that “time is running out to prepare for the next pandemic,” a point that he expanded on in his 2017 book, “Deadliest Enemy: Our War Against Killer Germs.”
He discussed the coronavirus at a recent online event organized by the New America think tank with me. The discussion was edited for length and clarity and updated with new information.
DR. MICHAEL OSTERHOLM:
As we learn more about the transmission of this virus, it’s very clear that it is at least, if not more, infectious than even what the world experienced in the historic pandemic influenza of 1918. And I’m convinced that this pandemic is following what we experienced in 1918.
While I don’t expect the Covid-19 pandemic to be exactly like that of 1918, the epidemiology tells me that this first wave of illness is, in fact, just the beginning of what could very easily be 16 to 18 months of substantial activity of this virus around the world, coming and going, wave after wave. Robert Redfield, the director of the Centers for the Disease Control (CDC) commented Tuesday that he believes a 2020-21 winter wave could be worse than what we have experienced this spring.
Will the next waves get bigger like they did in 1918 when there was a spring peak and a fall peak?
We don’t know that, but it surely is a virus that likely will have to infect at least 60 to 70% of the population before we see a major reduction in its transmission.
I think it’s very hard to realize that we’re first in the first innings of this crisis. A quote keeps coming back to me from Sir Winston Churchill: “This is not the end. It is not even the beginning of the end, but it’s perhaps the end of the beginning.” I think that’s where we’re at right now. You might say we’re in the second inning of a nine-inning game.
We’ve got to consider how we’re going to prepare ourselves for the possibility that some of the cities that have already been hit hard will have peaks some months down the road that may be much larger in case numbers than we’re seeing right now.
For several months, people kept pointing to Asia and saying, “If we just adopt the same response as China or Singapore or Japan, then we could bring this under control.” Finally, people are realizing that these comprehensive – some would consider them even extreme – control measures adopted in Asian nations are starting to show the breaks in their effectiveness.
Singapore has witnessed rapidly increasing transmission occurring in the community. The same thing has happened in Japan, which is now in a state of emergency. What’s even more confusing is what’s happening in China. We are seeing large public crowds in China again.
China is now reporting that most individuals who test positive for the coronavirus are asymptomatic.
Many health experts are very concerned that the Chinese government is not reporting all cases. After more than four months of some of the most extreme population movement limitations in modern history, we’re still seeing transmission occurring inside of China.
And as the Chinese government permits so many people in the Hubei province to go back to work, I’m very concerned that we’ll see increased transmission in other provinces of China. I don’t believe it will ever be as bad as it was in Wuhan in January, but we can’t use Asia as the perfect model for what control measures will work here. We are going to be dealing with Covid-19 on a global scale for months to come, trying our best to suppress it as much as possible.
What is our strategy in the US going forward? At this point, my biggest concern is that we still don’t have a national plan. We have to develop a comprehensive and effective national response to Covid-19.
BERGEN: What should that long-term strategy look like?
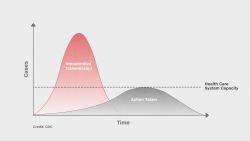
OSTERHOLM: The first step is to acknowledge the need for a long-term strategy. We’re so focused on “the here and now” of this issue – the idea of just getting over this wave and flattening this curve. And I agree with that. It’s an immediate issue, particularly if you are in one of the places that’s on fire right now like New York, Detroit, Chicago, New Orleans. But people have handled these local hot spots almost like they were faced with a hurricane that has now made landfall. Now we can get into remediation and recovery from this first round of crisis.
So, the first thing we need is a plan. That’s critical.
The second thing we need to address is: What is our long-term strategy? I believe we have really two choices at the edges and some additional options in between. One choice is to try to lock down our society and economy like Wuhan did. Most of us understand that adopting that approach means we’re not only destroying the economy but also destroying society as we know it.
The other alternative is to let viral transmission go willy-nilly until it burns through the population. I am strongly against that approach for two reasons. First, that would mean we could potentially experience millions of deaths just in the United States. It would bring down our health care system as we know it; it would mean severely compromised care for Covid-19 patients and fewer care options for anyone else with other serious health issue such as a heart attack, acute asthma attack, cancer or an injury from an accident. So, that is not a viable alternative.
There’s got to be an approach in the middle. I call it “threading the rope through the needle,” where we open our economy and everyday life in a way that is capable of rapidly detecting the emergence of new waves of infection. Then we do whatever we can again with physical distancing to limit the new infection’s spread.
By the way, I find the term “social distancing” unfortunate. It is physical distancing that we need in order to stop the virus transmission. Let’s never social distance. Let’s try in our modern age of the Internet, to do a better job with staying social.
So how do we get the younger, otherwise healthy demographic back to work, a group we know will be at much lower risk of serious disease and death if they get infected? How do we bring a substantial number of these individuals back into society and at the same time try to protect those who have the highest risk of a severe outcome? Remember we have to get them through the next 16 to 20 months, or until we get a safe and effective vaccine.
For those who are vulnerable, it is imperative that we minimize the risk of infection and the likelihood of ending up in a hospital and dying. And please know this approach will never be perfect; some younger people will get sick and even die. But the rate of serious illness and deaths will be many times lower for the young than for older individuals or those with underlying health risk factors.
Our strategy can’t be the outcomes of day-to-day press conferences. It can’t be 30-day plans to “social” or “physically” distance. It’s got to address how we’re going to incorporate day-to-day prevention actions, and what we ask the public to do must be realistic.
For example, everybody wants to do widescale coronavirus testing today. Talking heads without any experience in testing declare, “We’ll test millions of people each week, and then we’ll know who is infected and can follow up.” Very few people realize that the testing community in this country can’t do that. We don’t have adequate international manufacturing capacity and supply chains for reagents, the chemicals needed to run these tests.
The reagent capability – meaning securing those chemicals that are key for running many of these tests, whether you’re testing for virus or antibody – before the pandemic was more or less, adequately supported by a “garden hose of production.” Then Covid-19 came along and the Asian countries, specifically China, demanded a major increase in reagent supplies.
Finally, the whole world caught the pandemic, and now there are billions of people who need to be tested. We need a firehose to meet that demand but we can’t build reagent manufacturing facilities overnight. I urge that whatever we do going forward has to be based on reality. We’re not going to test your way out of this thing when we don’t have tests.
I paraphrase a quote from former US Secretary of Defense (Donald) Rumsfeld who said, “When you go to war, you don’t get to go with what you want. You have to go with what you have.”
So, we’re going to have this reagent issue for some time to come, and we must understand that and come up with a plan based on reality.
BERGEN: What is the role of the reagents in these tests?
OSTERHOLM: Reagents in the test are like the gasoline in a car. For example, if you take a nasal swab from a possible Covid-19 case, you have to extract specific material out of that swab. So, if you don’t have the chemical reagent to do that, you can’t run the test. You just can’t have a swab and walk into a lab and say, “Test this.” For each test, there are chemicals required to run it, and it varies by which kind of test you’re talking about.
BERGEN: You mentioned the 1918 pandemic in which some 50 million people died. I presume that public health generally has improved since then?
OSTERHOLM: I surely don’t want to suggest that the number of people who died in 1918 is the number we might expect with this novel coronavirus pandemic. Today, of course, we have a much larger population globally than we had back then. But I think that the epidemiology is following the trend of the 1918 pandemic, with the exception, of course, that in 1918 those who died were more often in the younger adult age population than we’re seeing today.
We should remember that the current pandemic is caused by a coronavirus and not an influenza virus like was the case in 1918. History will tell if the two act very much the same way in terms of the epidemiology of the diseases.
'Unseen Enemy: Pandemic'
One issue is that, except for social distancing, we don’t have any other major public health tools to fight the virus. Even if we get effective drugs, which would surely be a godsend, that is not going to stop virus transmission. These drugs, if available on an international level, would lessen the impact of the pandemic in terms of numbers of severe cases and deaths. Transmission will still continue, as most of it is occurring early on in the illness before you would even start taking drugs.
BERGEN: You mentioned the University of Washington model, which seems to have been influential in the White House. But Muriel Bowser, the Mayor of Washington, DC, for instance, is using different models – one from the University of Pennsylvania, to evaluate the pandemic, and she has said that Covid-19 could peak in DC at the end of May. This is a very different conclusion than the mid-April peak suggested by the University of Washington model.
Shouldn’t it be the CDC’s job to come up with a nationally agreed upon model to evaluate the situation? No matter how good these individual universities are, local leaders are essentially shopping around for models that can vary from state to state or federal government to local government.
OSTERHOLM: The CDC’s absence in this pandemic in the United States has been, I think, a tragedy. Yes, we’re all well aware of the fact that there were problems with the rollout of testing early on. But there are some of the best minds in the business in the areas of preparedness and pandemic response at the CDC, and their inaction in coordinating all of these modeling activities in a way that we can synthesize them is really unfortunate. If I could urge any one thing happen today in the federal response, it would be to give the CDC a much more important role at the table than it currently has.
Right now, on the coronavirus task force, there is no primary public health expert member. I think Dr. Anthony Fauci has done an incredible job of representing the infectious disease perspective. I have the highest regard for him and thank God he’s been there. But with regard to the issue of modeling and the issue of surveillance, that expertise is at the CDC.
I’ve come to the point of concluding, let’s throw out all the models. They’re not helpful because they’re causing some to believe the administration is overinflating the numbers of potential cases and deaths. Meanwhile, others conclude the model used by the White House is intentionally underreporting the numbers and they think the administration is trying to downplay this pandemic. It seems that nobody trusts anybody.
I’m from rural Iowa where a lot of very commonsense, smart people live. I think to myself: if I were at the local café, how could I explain what’s going on to a group of people sitting at that table? I’d say to them, let’s just take the following simple numbers.

There are 320 million people in the United States. If half of them get infected in the next 6 to 18 months, that’s 160 million people. The 50% rate of infection over the course of the pandemic is at the low end of my colleagues’ consensus on what we can expect to see given the infectiousness of this virus.
Based on what we know from Asia, from the European Union and from the United States, about 80% of these cases will have asymptomatic, mild or moderate illness but won’t need professional medical care. About 20% of infected people will seek medical care. That’s 32 million people.
Of those, about half will be hospitalized. That’s 16 million people. Of those who are hospitalized, about half will actually require some form of critical care. That’s 8 million people. About 0.5 to 1% of the total number of 160 million infected people will die. So you have the possibility of at least 800,000 deaths in the US over the next 18 months. This is the number of deaths I’m expecting.
If you don’t like the numbers I just used, go ahead and change them however you want. Just provide your justification. We have a long way to go with this pandemic. We just need to make people understand that this is going to be bad until we get a safe, effective and widely available vaccine. It’s a sad commentary about our state of affairs that the number of people who die from Covid-19 in the US ranks as one of the top daily causes of death – on some days it’s been ranked higher than heart disease, cancer and accidents. Six weeks ago, it wasn’t even in the top 60 causes of deaths.
What I’m trying to get people to understand is that a model is just a model, and we’re putting way too much weight on its ability to estimate with precision where this pandemic is going. What we need is a general sense: Is this a Category 2, a Category 5, or a brand new category called a Category 8?
No matter how you slice it, on the most basic back-of-the-envelope estimate, this is a really bad situation. So, we have to be prepared for that.
BERGEN: Is there a world in which we would all be issued nationally recognized status as immune that would allow us to go back to work? Relatedly, would that really work if there are faulty tests?
OSTERHOLM: I’ve seen this idea expressed by a number of people in the past few days. They believe that we just need to have a kind of system where we see if you have been infected using antibody tests. Right now, Covid-19 virus and antibody testing in this country and in some other parts of the world is nothing more than the Wild, Wild West.
Before we can launch on any kind of an immune status national program, we have to understand two things. One is what the test results really mean. Does a positive antibody test mean someone has immunity or not? I think that’s a big challenge. In a low prevalence area for previous Covid-19 infection, which is most of the country, a positive antibody result could be a true positive or a false negative.
These both are important moonshot issues and we need to do the work right now to clarify. We need to invest in developing critical manufacturing infrastructure for reagents and support testing in general. And then, second of all, we have to know what that testing means.
I think there have been a number of health care workers who have been infected or who suspect they’ve been infected, but were never tested at the time. There wasn’t adequate testing available. Today if they could know that they were antibody-positive and there was sufficient data to support that they likely were protected against becoming infected again, then, wow! Think how that would change the picture of health care if 20 or 30% of our current medical staff were already protected. That would give them an incredible peace of mind.
The problem is that we don’t have a national prioritization around this issue.
BERGEN: Why did the US fail to have an adequate supply of personal protection equipment (PPE)? Is it a policy failure, or is it something else?
OSTERHOLM: Well, I think it’s a combination of several things. First of all, we did not anticipate this situation, and when you look at a strategic national stockpile that may have a tiny portion of the N-95 masks needed for the country, that’s hardly a stockpile. That’s not even a good late night stopover.

Right now, we’ve put 50 different governors in charge of the country, and I think many of them have performed admirably. They’re trying to thread that rope through the needle, and they are pretty much on their own.
Logistically, why are governors suddenly entering the private procurement market? As you’ve likely heard many times, we’ve basically directed the 50 states into an eBay-like environment where every state or major city has to outbid every other state or city to get critically needed supplies. That is crazy.
So what we need to do is come up with a standard. Which state should be the highest priority for ventilators and why? Which has the highest priority for PPE and why? And then we should match up inventory with that priority list. If we don’t have enough for each state’s need, then at least there’s transparency. Maybe resources didn’t show up in a particular state, but it wasn’t because that state couldn’t pay the most or wasn’t savvy enough to have a relationship with a private sector company.
Right now I liken the situation to this: we’ve got 50 pilots all landing their planes at the same time all by themselves, and only if they’re prepared to have a head-on collision with other planes do they get the chance to call the air traffic control tower. That’s unacceptable, and that’s what’s happening.
BERGEN: Now that we know that the virus is, to some extent, transmitted through droplets in the air, what is the relative risk of going to grocery stores, pharmacies and other necessary public places? Should we be ordering delivery or requesting curbside pickup? If most people in the store are wearing masks, is it safe to go?
OSTERHOLM: This is a huge challenge and a tough question to answer.
We have to acknowledge that we have put far too much emphasis on hand washing and environmental control. I come from a world of infectious diseases where I’ve spent my whole life preaching the importance of hand washing. It is important. But we have to be intellectually and scientifically honest with the public and admit that, while we shouldn’t we stop washing our hands, we also shouldn’t assume that decontaminating the environment or washing our hands is going to be enough to prevent us from becoming infected.
This virus could be in the air around infected people. It could be the same air we share and breathe. The more times you go into public spaces, the greater the likelihood you’re going to swap some air with somebody who has the virus and doesn’t even know it. Again, we have to be honest about that.
Does that mean you shouldn’t go to the grocery store? Well, I would say if you’re a person of high risk for a serious disease outcome, you should do everything you can to find a way to get those groceries delivered to you, even left outside your front door where you can go pick them up and not have to have contact with someone.
Now, for others who say, “Well, you know what? I’m at a relatively low risk of having a serious outcome if I do get infected,” you still have to think about whether you might be transmitting that infection to others. I think we have to be more honest and just say that, yes, breathing someone else’s air is going to put you at risk. On any one given day, how big of a risk is that? I don’t know.
We can’t stop living life. We have to move forward. But we must do so while thinking about how to get people back into society in a way that is thoughtful and takes into account every possible option to make sure people don’t get seriously ill and don’t subsequently die.